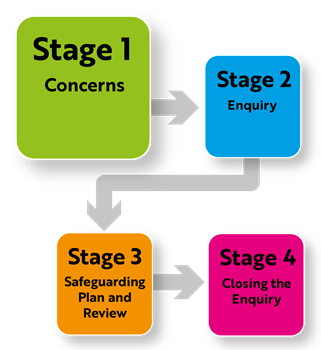
Stage 1 - Concerns: Advice for Submitting an Adult Safeguarding Concern
 1. What is abuse and neglect?
1. What is abuse and neglect?
There are many forms and ways that adult abuse and neglect can occur, so we should not be constrained by definitions and terminologies. Adult abuse is also often complex involving more than one type of abuse occurring at any one time.
Abuse or neglect is any behaviour towards a person that deliberately or unknowingly causes him or her harm, endangers their life or violates their rights. This may be the result of deliberate intent, negligence, or ignorance. Exploitation can be a common theme in the experience of abuse or neglect. Whilst it is acknowledged that abuse or neglect can take different forms, the Care Act guidance identifies the following types of abuse or neglect:
Physical Abuse
Including assault, hitting, slapping, pushing, misuse of medication, restraint, or inappropriate physical sanctions.
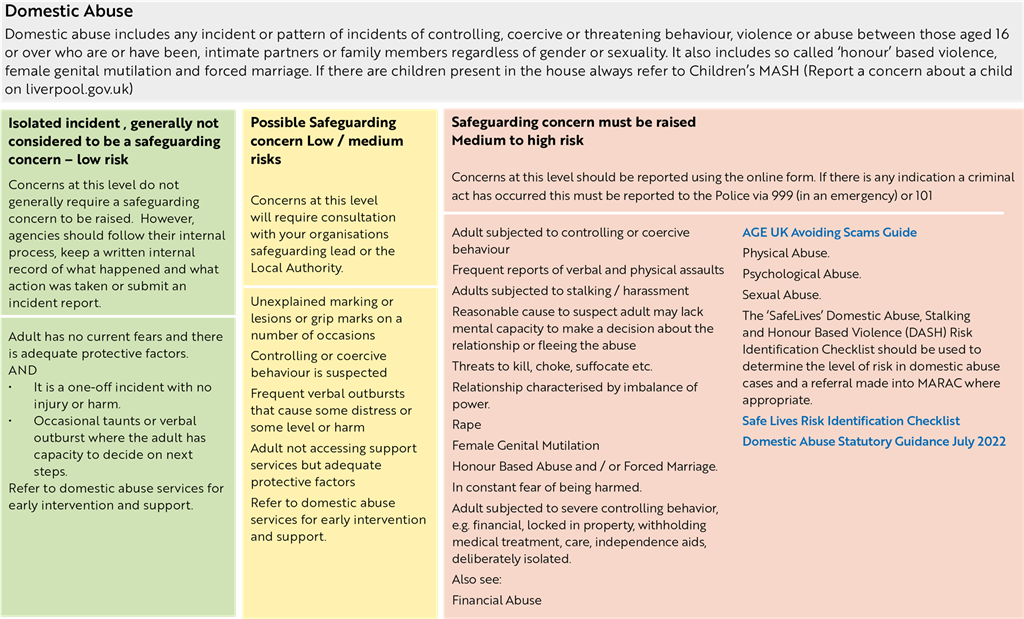
Domestic Abuse
Including psychological, physical, sexual, financial, emotional abuse, and so called ‘honour’ based violence.
Definition: Any incident or pattern of incidents of controlling, coercive or threatening behaviour, violence, or abuse between those aged 16 or over who are or have been intimate partners or family members regardless of gender or sexuality. This can encompass, but is not limited to psychological, physical, sexual, financial, and emotional abuse.
This definition includes so-called ‘honour’ based violence, forced marriage and female genital mutilation (FGM). It also covers a range of different types of domestic abuse including coercive control.
Merseyside Risk Identification Toolkit (MeRIT) is widely used in Merseyside to allow us to clearly understand the nature of domestic abuse incidents to gain an understanding of the level of risk of harm that the victim is experiencing. It consists of 40 questions aimed at gathering information, including on the background of the relationship and also what happened leading up to and during the incident.
Multi-Agency Risk Assessment Conference (MARAC) is a regular meeting where local organisations share information about high-risk domestic abuse victims with the aim to develop risk focused, coordinated safety plans to support victims and their children which manages risk and increases safety.
To access MeRIT forms, please visit:
https://liverpool.gov.uk/referrals/professionals-refer-high-risk-victims-of-domestic-abuse/
Domestic Abuse and Suicide
Learning from several Domestic Homicide Reviews where suicide has been the cause of death linked to domestic abuse, has highlighted the need for professionals to be more aware of factors or experiences which can increase risk of suicide.
These include:
- Life-threatening abuse
- Sexual assault
- Childhood trauma
- Coercion and Control
- Multiple or repeated abuses
- Harmful coping strategies such as self-harm, drug abuse, alcohol abuse
- Feelings of despair and hopelessness relating to abuse
- Breakdown of positive relationships (Including where individuals no longer have contact with their children or where contact is ‘controlled’ by the child’s carer).
- Lack of access to support
- Escalation of abuse / rapid escalation / rapid escalation of other risk factors
- Sleep deprivation
Useful links
Learning Legacies
Domestic Abuse and Suicidality Briefing can be found here.
Jane Monckton Smith 8 stages can be found here.
Services
Amparo – free emotional and practical support for anyone impacted in any way by death from suicide, provided whenever, wherever, and however it is needed.
Reach Out Liverpool – campaign and resources designed to help people having thoughts of suicide to get help and to help people concerned about someone to know how to help.
Zero Suicide Alliance – training and support for individuals and organisations to support suicide awareness and prevention.
The Life Rooms – helping people to access support to address a wide range of factors that impact mental health as well as offering opportunities for learning and connection through local events.
Kind to Your Mind Liverpool – campaign and resources designed to help people in Liverpool gain a greater understanding of their mental health, how to feel better and access support when needed.
Hub of Hope - national signposting tool featuring local, national, peer, community, charity, private and NHS mental health support and services.
Liverpool CAMHS – Local hub of information and support for children and young people’s mental health.
WHISC – Support, therapy, workshops, classes and training courses to support women’s wellbeing and mental health.
For a more comprehensive definition, please refer to Domestic Abuse Act 2021:
Domestic Abuse Act 2021 Statutory Guidance
Link to Liverpool Domestic Abuse Providers
https://liverpool.gov.uk/communities-and-safety/crime-and-safety/domestic-abuse/
Gaslighting
Watch these two short clips for examples of “Gaslighting” a common form of abuse seen in Domestic Abuse:
Gaslight - You Think I'm Insane: After becoming hysterical at a friend's house Paula (Ingrid Bergman), Gregory (Charles Boyer) shares his frustrations with her.
Gaslight (1944) - You Think I'm Insane Scene (5/8) | Movieclips – Youtube
Gaslight - You're Being Driven Insane: With Brian's (Joseph Cotten) help, Paula (Ingrid Bergman) discovers the horrifying truth about her husband.
Gaslight (1944) - You're Being Driven Insane Scene (6/8) | Movieclips - Youtube
Honour-based Abuse (HBA) and Harmful Practices
Savera UK Learning Hub resources: https://www.saverauklearninghub.co.uk/.
Free online training for Female Genital Mutilation and Forced Marriage: Virtual College.
Coercive Control
Stalking
Merseyside Domestic Violence Service (MDVS) have a specialist Stalking Support Service: https://www.mdvs.org/stalking-services/Call 07802 722 703 or email info@mdvs.org
In an emergency, call 999
For other support you can contact the National Stalking Helpline: 0808 802 0300 Open 09:30 to 20:00 Mondays and Wednesdays and 9:30 to 16:00 Tuesdays, Thursdays, and Fridays.
www.stalkinghelpline.org Enquiry form
Alice Ruggles Trust Stalking Video SD360p (youtube.com)
Paladin - Get Support (paladinservice.co.uk)
Paladin National Stalking Advocacy Service Referral Form (Page 1 of 6) (office.com)
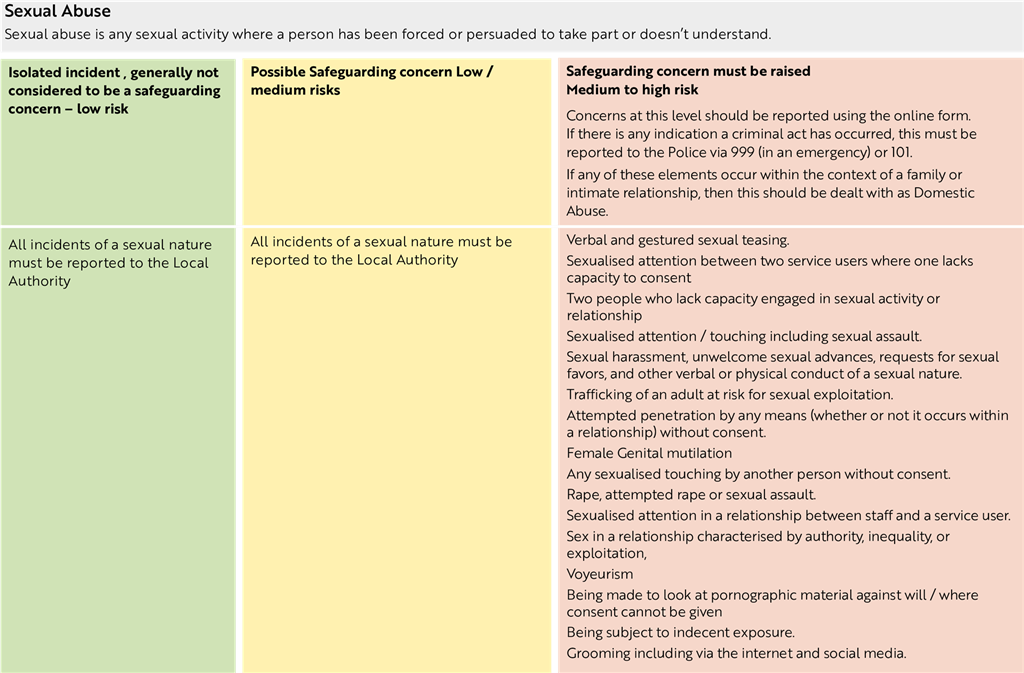
Sexual Abuse
Including rape, indecent exposure, sexual harassment, inappropriate looking or touching, sexual teasing or innuendo, sexual photography, subjection to pornography or witnessing sexual acts, indecent exposure and sexual assault or sexual acts to which the adult has not consented or was pressured into consenting.
RASSO Booklet pdf
Sex Worker Exploitation
Changing Lives: STAGE project – Poster: The Journey of a woman experiencing sexual exploitation https://www.changing-lives.org.uk/policy-and-research/stage-project
STAGE have developed a a toolkit for professionals to navigate information quickly for women who have unmet needs and have experienced trauma: https://changinglives.cdn.prismic.io/changinglives/17c030a2-1c9c-48dd-968e-ad965a666e2f_STAGE+Toolkit.pdf
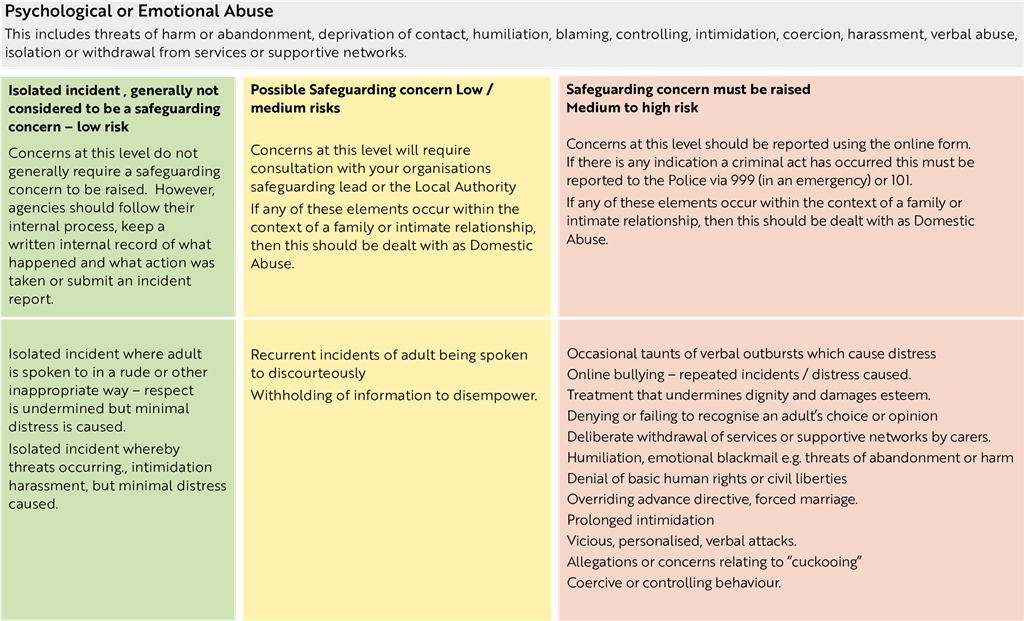
Psychological Abuse
Including emotional abuse, threats of harm or abandonment, deprivation of contact, humiliation, blaming, controlling, intimidation, coercion, harassment, verbal abuse, cyber bullying, isolation or unreasonable and unjustified withdrawal of services or supportive networks’.
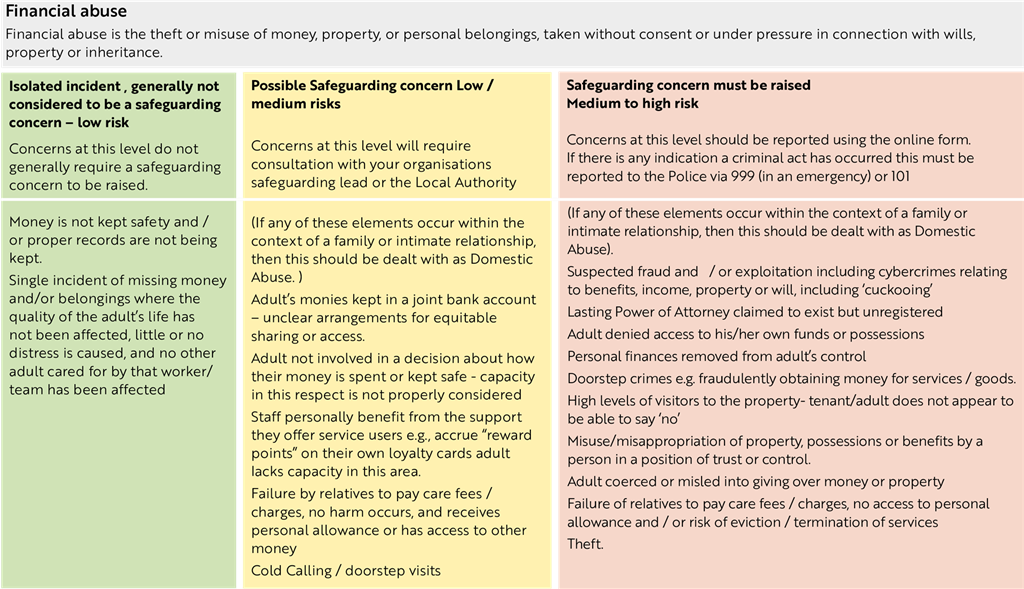
Financial or Material Abuse
Including theft, fraud, internet scamming, coercion in relation to an adult’s financial arrangements, including in connection with wills, property, inheritance or financial transactions, the misuse or misappropriation of property, possession, or benefits.
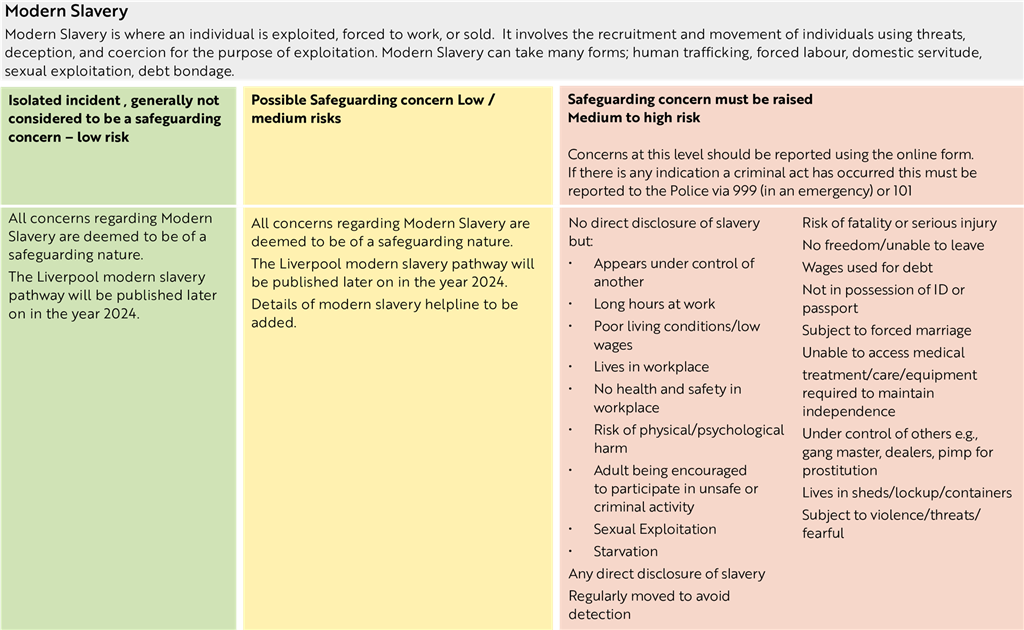
Modern Slavery
Slavery, human trafficking, forced labour and domestic servitude, traffickers and slave masters using whatever means they have at their disposal to coerce, deceive and force people into a life of abuse, servitude and inhuman treatment.
Merseyside Modern Slavery and Human Trafficking Strategy 2024-2028 https://www.merseysidepcc.info/media/nnigc1yf/a4-modern-slavery-final.pdf
Types of Modern Slavery and Human Trafficking:
Domestic Servitude
Someone is forced to work in someone else’s home with little freedom or pay. This could involve cooking, cleaning, looking after children, etc.
Sexual Exploitation
Victims are forced to perform sexual acts.
Criminal Exploitation
Someone is forced into crime such as carrying drugs, forced begging, theft, or fraud. Adults who are most vulnerable to criminal exploitation may use drugs, are in financial difficulty or have mental health problems are at greatest risk of being criminally exploited and becoming involved in county lines exploitation or Cuckooing. County lines is the name given to drug dealing where organised criminal groups (OCGs) use phone lines to move and supply drugs, usually from cities into smaller towns and rural areas.
Young adults who have just turned 18 may have been criminally exploited as a child and may continue to be exploited.
What to do if you have concerns about someone over the age of 18 being a victim of criminal exploitation?
If you’re concerned about drug-related crime in your area or think someone may be a victim of drug exploitation, please call us on 101. If it’s an emergency, please call 999.
Exploitation known as ‘Mate crime’
The term Mate Crime is generally understood to refer to the befriending of people who are perceived by perpetrators to be vulnerable for the purpose of taking advantage of/exploiting and/or abusing them.
Please see this short video: Tricky friends https://youtu.be/tEx8uFuNZGU
Cuckooing
When one person takes over another person’s home and uses it for their own illegal or immoral purposes. Uses of the home can be for growing a cannabis farm, breeding dogs, selling drugs etc. The actual person whose home it is may be forced to clean and work for the person who has taken it over with access to money or movement being restricted.
Cuckooing 7-min Briefing Word document
Forced Labour
According to the ILO Forced Labour Convention, 1930 (No. 29), forced or compulsory labour is:
All work or service which is exacted from any person under the threat of a penalty and for which the person has not offered himself or herself voluntarily.
Debt Bondage
According to Unseen, ‘Debt bondage is a form of forced labour and happens when a person is forced to work to pay off a debt. They are tricked into working for little or no pay, with no control over their debt. This is thought to be the most widespread form of slavery today.’
Forced Scamming
International Justice Mission outlines that Forced Scamming is a fast-growing form of modern slavery and human trafficking.
This can often involve:
- A victim recruited via a convincing fake job advert (often abroad) and trafficked into a heavily guarded compound.
- Once at the compound, traffickers take the victim’s passport and phone. They are trapped and unable to leave.
- The victim is forced to conduct scams for up to 20 hours a day, six days a week.
- The victim often experiences extreme violence including electrocution or torture.
Spiritual Abuse / Abuse linked to witchcraft
Where accusations and claims of witchcraft or spiritual possession are used to control victims into Modern Slavery through fear.
Forced Marriage
Unseen defines this as “Someone who is married against their will and can’t leave. Most child marriages can be considered slavery.”
Further guidance on forced marriage can be found here
https://www.gov.uk/guidance/forced-marriage
A forced marriage is where one or both people do not or cannot consent to the marriage and pressure or abuse is used to force them into the marriage. It is also when anything is done to make someone marry before they turn 18, even if there is no pressure or abuse.
Forced marriage is illegal in the UK. It is a form of domestic abuse and a serious abuse of human rights.
The pressure put on people to marry against their will may be:
- physical: for example, threats, physical violence or sexual violence
- emotional and psychological: for example, making someone feel like they are bringing ‘shame’ on their family
- Financial abuse, for example taking someone’s wages, may also be a factor.
- The Anti-social Behaviour, Crime and Policing Act 2014 made it a criminal offence in England, Wales and Scotland to force someone to marry. (It is a criminal offence in Northern Ireland under separate legislation).
This includes:
- taking someone overseas to force them to marry (whether or not the forced marriage takes place)
- doing anything intended to cause a child to marry before their eighteenth birthday, whether or not a form of coercion is used
- causing someone who lacks the mental capacity to consent to marry to get married (whether they are pressured to or not)
There is also information with this guidance on how to contact the Forced Marriage Unit and how they can help.
The Forced Marriage Unit has created a guidance document which comprises:
- multi-agency statutory guidance for dealing with forced marriage, which provides guidance for every person and organisation that has a public function relating to safeguarding and promoting the welfare of children and vulnerable adults; and
- multi-agency (non-statutory) practice guidelines on handling cases of forced marriage, for frontline workers, including health professionals, educational staff, police, children’s social care, adult social services, local authority housing staff, registrars, and staff working at the UK border.”
Organ Harvesting
The Modern Slavery Act defines this as when victims are trafficked for their internal organs (typically kidneys or liver) to be harvested for transplant.
Get support for suspected Modern Slavery
Unseen, who provide the Modern Slavery helpline, are part of the Network and an integral partner who support thousands of people every year in various ways, from direct support to victims, to advice to someone who thinks they have spotted incidents of Modern Slavery.
There is more information available here:
https://www.gov.uk/government/publications/human-trafficking-victims-referral-and-assessment-forms/guidance-on-the-national-referral-mechanism-for-potential-adult-victims-of-modern-slavery-england-and-wales
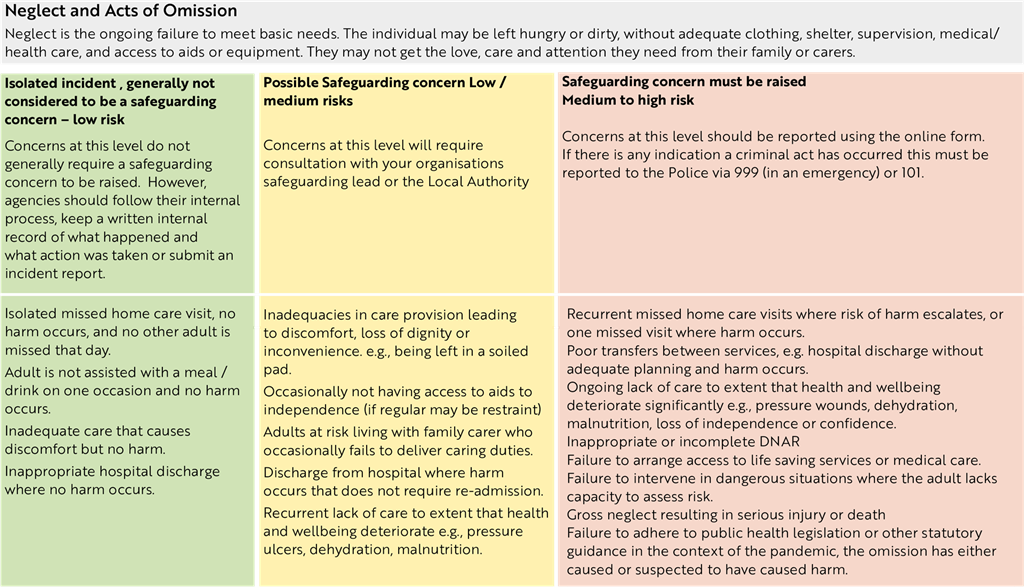
Neglect and Acts of Omission
Including ignoring medical, emotional, or physical needs, failure to provide access to appropriate health, care and support or educational services, the withholding of the necessities of life, such as medication, adequate nutrition, or heating.
Nice Guidelines: Safeguarding in Care Homes
Below is further guidance in relation to neglect:
Safeguarding concern and pressure area care
Pressure ulcers are not always due to poor care and neglect, so each individual case should be considered independently, considering the person’s medical condition, prognosis and any underlying skin conditions. The person’s mental capacity to agree to their care must also be assessed where appropriate. Records should be kept of the person’s compliance with their care plan as well as any best interest decision, where the person lacks capacity.
A safeguarding concern should be raised when a failure to provide adequate care has resulted in a person developing a pressure ulcer; this would include circumstances such as: failure to seek specialist advice, appropriate equipment not provided in a timely manner and care plan/repositioning charts not in situ. The safeguarding adults protocol advises that the safeguarding decision guide is completed by a qualified nurse (immediately or within 48 hours of identifying the pressure ulcer) and a safeguarding concern is raised when there is a score of 15 or above. However, this should not replace professional judgement. A copy of the completed decision tool should be sent alongside the safeguarding concern and a copy should be kept on the person’s file. If a safeguarding concern is not required, the decision tool should be retained on the person’s file. Please see the guidance via this link:
Safeguarding adults protocol: pressure ulcers and raising a safeguarding concern - GOV.UK (www.gov.uk)
Skin damage that is established to be because of incontinence and/or moisture alone should not be recorded in the notes as a pressure ulcer but should be referred to as a moisture lesion to distinguish it and recorded separately. However, this might be because of neglect or poor oversight and thus, it should be explored not ignored.
The National Wound Care Strategy Programme offer clear advice to health and care practitioners about the fundamentals of evidence informed care for people who have or are at risk of developing pressure ulcers. The document below highlights a pathway of care promoting early risk identification.
National wound care strategy programme
https://www.england.nhs.uk/pressure-ulcers-revised-definition-and-measurement-framework/
NHS Improvement ‘Pressure Ulcers: Revised definition and Measurement’:
To note, there are national requirements to report pressure ulcers. All category 3 and 4 ulcers that meet the criteria under the Patient Safety Incident Response Framework [PSIRF], this new approach is a change in health from the Serious Incident Framework [2015] and a significant step towards establishing a safety management system across the NHS.
https://www.england.nhs.uk/publication/patient-safety-incident-response-framework-and-supporting-guidance
There is also the Cheshire & Merseyside Regional Pressure Ulcer Policy V3 January 2024 to refer to as well as agencies own Pressure Ulcer Organisations guidelines and policies.
Cheshire Merseyside Regional PDF
Other helpful links are available:
Pressure ulcers: how to safeguard adults
Stop the Pressure: NHS Improvement
Guidance for reporting Falls as Adult Safeguarding Concerns
There needs to be a shared understanding that falls happen, and it is not possible to prevent all falls. Where individuals are at risk of falls and/or have fallen then a falls risk assessment is undertaken. This should be completed in conjunction with the individual and an agreed, shared plan in place. Where there are concerns about an individual’s mental capacity to make decisions in relation to their care and support, capacity must be assessed under the Mental Capacity Act and, if they do lack capacity, a best interests decision can be made around the care plan that is required to keep them safe. All assessments and outcomes must be recorded in the person’s care folder.
When a fall should be reported as a safeguarding concern (a concern about possible abuse/neglect by another person and not because there is a general concern about a person’s safety):
- Where a person sustains an injury due to fall and there is concern that a risk assessment is not in place or was not followed, then this must be reported as a safeguarding concern because the person has experienced avoidable harm and amounts to neglect on the part of the care provider.
- Where a person has sustained an injury which has resulted in a change of function and appropriate medical attention has not been sought, this must be reported as a safeguarding concern.
- Where a person has an unexplained injury, other than a very minor injury, this must be reported as a safeguarding concern.
When a fall is not a safeguarding concern (accidental falls where a risk assessment is in place and followed):
- When a person is found on the floor, is not injured and appropriate risk assessment is in place and has been followed.
- A fall is witnessed, and appropriate risk assessment is in place and has been followed.
- A person states they have fallen and have the capacity to make decisions in relation to their care and support.
There has been some understanding from providers that they should report all unwitnessed falls as safeguarding concerns, but this should not be the case; it should be based on professional judgement assessing the circumstances of the event. Therefore, for example, if a person has an ‘unwitnessed fall’ where they stated they fell and explained what happened and a risk assessment is in place which has been followed then it is likely that abuse/neglect has not occurred. However, for all unwitnessed falls, specific post fall neurological clinical monitoring should be undertaken. There is guidance linked to NICE (The National Institute for Health and Care Excellence) and NPSA (National Patient Safety Agency).
In circumstances where a person has sustained an injury the manager on duty should use judgement based on the evidence available to determine what may have happened. If the person has an injury, other than a minor injury, which cannot be explained than this should be referred as a safeguarding concern. If in doubt, raise a safeguarding concern.
To note, providers must consider their responsibilities to report under RIDDOR (Reporting of Injuries, Diseases and Dangerous Occurrences Regulations) as well as considering if a fall is a safeguarding concern or a care concern. For example, where a fall has arisen out of or in connection with a work activity and results in a specified injury such as:
When to report a safeguarding concern about medication
The National Patient Safety Agency (NPSA) define a medication error as an error in the process of prescribing, dispensing, preparing, administering, monitoring, or providing medicine advice, regardless of whether any harm occurred. Therefore, in terms of whether a medication error needs to be reported as a safeguarding concern, the provider needs to decide if a medication error as defined above has occurred and in addition if there is evidence of significant impact upon or significant harm to the individual person subject to the error. Otherwise, the error should be reported and recorded in accordance with medication and management of incidents policies and procedures (see also NICE Guidance NICE and consideration of reporting a care concern.
Care home providers should ensure that a robust process is in place for identifying, and reporting medication errors in line with the local authority safeguarding processes.
Medication incidents have several causes, such as lack of knowledge, failure to adhere to system and protocols, interruptions, staff competency, poor handwriting and instruction, poor communication, lack of training or basic human error. Different examples of what could be considered under safeguarding are:
> Adverse effects causing significant harm due to wrong medication or incorrect dose being administered.
> Malicious intent to cause harm.
> People left without pain relief resulting in a prolonged period of pain.
> Use of medication to control behaviour or restrict an individual
> Same drug being omitted repeatedly.
> Same carer repeatedly failing to administer medication appropriately.
> Omissions of antimicrobials resulting in delayed treatment
A safeguarding concern should always be raised when medication has been administered covertly without appropriate due consideration to the Mental Capacity Act 2005, Best Interest Decision process and administration plan to ensure medication is administered safely Refer to Covert Medication Guidance on NICE Covert medicines administration.
Where there are systemic failings which leads to repeated medication errors, a safeguarding concern should be raised under organisational abuse. Where an error is due to external factors or services e.g. pharmacy error, mismanagement by family, hospital discharge, GP prescribing etc., there is an obligation on all services to identify the failing and ensure the issue is addressed. This can be done through contacting the appropriate services to support a resolution such as the GP, Patient Safety, Social Worker, family members etc.
When reporting a safeguarding concern, the provider needs to ensure that there is the specific detail of the medication error such as name of medication, dose, timings, administration, impact on person and actions taken including if medical attention was sought.
Incidents related to controlled drugs (including loss or theft) need to be reported to your local NHS Controlled Drugs Accountable Officer (CDAO) at NHS England. You should also report incidents to the police (if necessary).
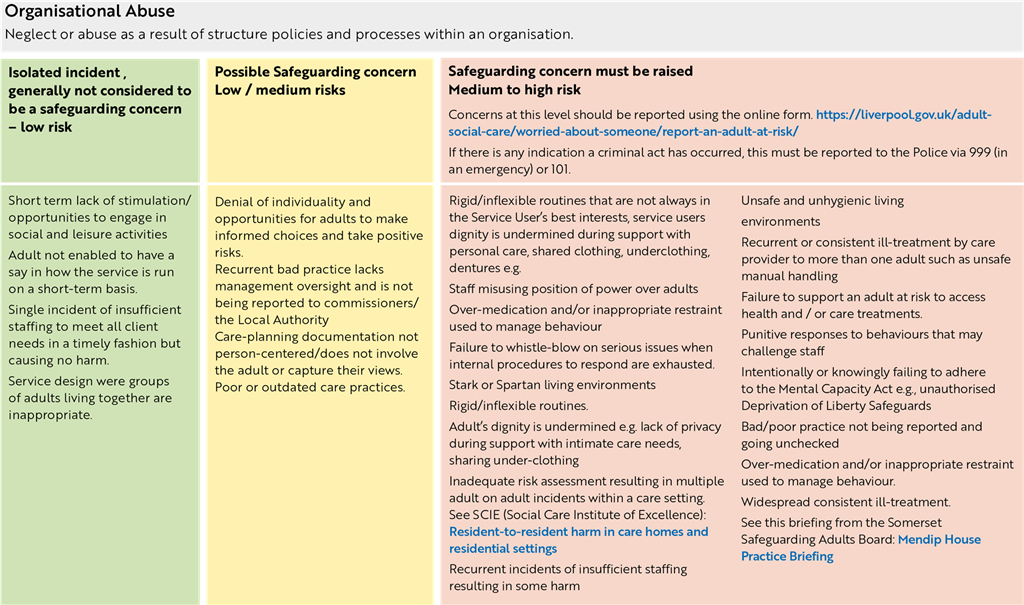
Organisational Abuse
Including neglect and poor care practice within an institution or specific care setting such as hospital or care home for example, or in relation to care provided in a person’s own home. This may range from one off incidents to on-going ill-treatment. It can be through neglect or poor professional practice because of the structure, policies, processes and practices within the organisation.
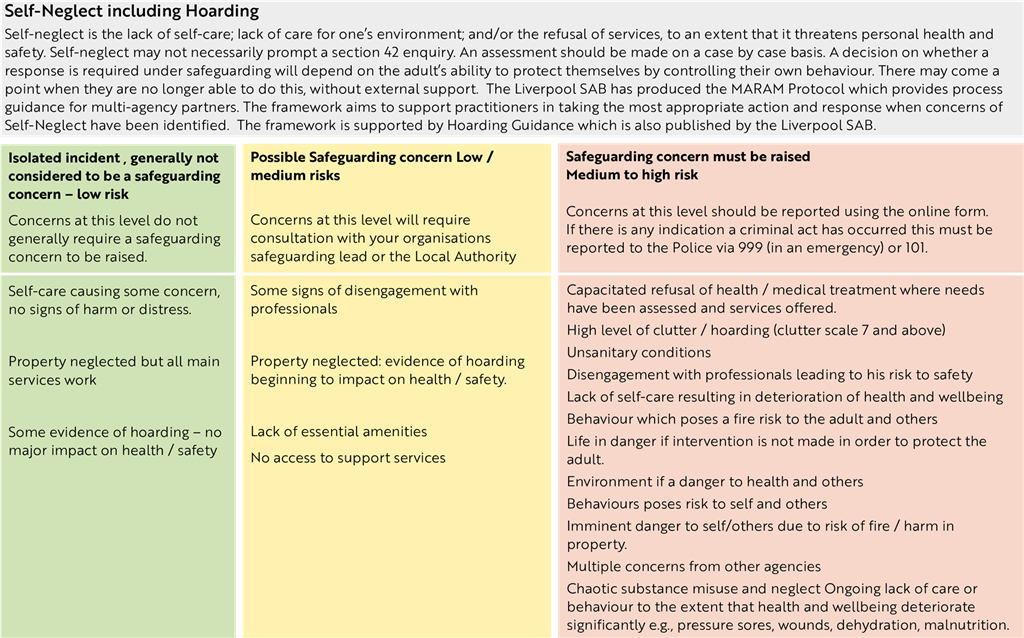
Self Neglect
Covers a wide range of behaviour around neglecting to care for one’s own personal hygiene, health or surroundings. It should be noted that self-neglect may not always prompt a section 42 enquiry. An assessment should be made on a case-by-case basis. A decision on whether a response is required under safeguarding procedures will depend on the adult’s ability to protect themselves by controlling their own behaviour. There may come a point when they are no longer able to do this, without external support. This may include hoarding when the hoarding becomes a serious risk to an adult with care and support needs.
Source: Chapter 14.17 Care Act Statutory Guidance
See link to Liverpool hoarding protocol for further guidance:
Liverpool Safeguarding Adults Board Multi Agency Policies and Guidance
See also the link for the Liverpool MARAM process.
Liverpool Safeguarding Adults Board Multi Agency Policies and Guidance
Self-Harm
Self-harm is different to self-neglect as self-harm is the deliberate act of injuring oneself whereas self-neglect is a lack of self-care that threatens personal health and safety. NICE (2022) refer to the term self-harm as any act of self-poisoning or self-injury carried out by a person, irrespective of the apparent purpose of the act (NICE Self-Harm Quality Standard). This commonly involves self-poisoning with medication or self-injury by cutting. Concerns of self-harm, therefore, do not come under the definition of a safeguarding concern (unless there are other additional factors such as self-neglect concerns) and instead if there are concerns that a person is self-harming frequently and there is a significant risk of accidental death, then they should be referred to mental health services for an assessment.
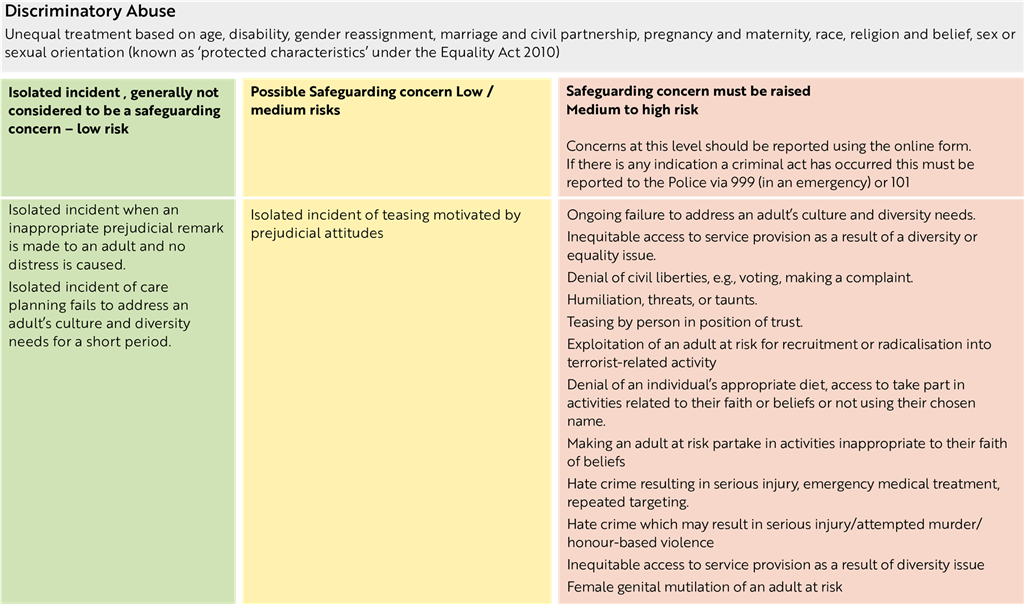
Discriminatory Abuse
Including harassment, slurs or similar treatment because of race, gender and gender identity, age, disability, sexual orientation, or religion.
For more information, please refer to: Discriminatory Abuse Webinar
All referrals must be sent, via e-mail, to prevent@merseyside.police.uk add referral form and referral guidance.
Hate Crime
Crimes committed against someone because of their disability, gender identity, race, religion or belief, or sexual orientation are hate crimes and should be reported to the police.
Click on the link below for further information:
https://www.gov.uk/report-hate-crime
https://www.stophateuk.org/
Merseyside Police Hate Crime
https://www.merseyside.police.uk/advice/advice-and-information/hco/hate-crime/what-is-hate-crime/
https://www.merseyside.police.uk/advice/advice-and-information/hco/hate-crime/how-to-report-hate-crime/
Hate Crime A5 leaflet (002) pdf
This is not an exhaustive list, there can be other types of abuse which may include:
Loan Sharks/Illegal Money Lending
Illegal money lenders are people who lend money illegally without the correct authorisation from the Financial Conduct Authority (FCA) required by the Financial Services and Marking Act 2000. Illegal money lenders normally appear friendly at first, but this behaviour soon changes once money is owed. A typical loan shark traps victims into a never-ending spiral of debt, sometimes exorbitant rates of interest and extra charges and may use threats and violence to frighten people who cannot pay back the money they have borrowed.
Referral and how to seek support
> Contact Stop Loan Sharks online https://www.stoploansharks.co.uk/ where you will find an online ‘report it’ form, live chat function, and information on how to get support for your client or your organisation and report a loan shark.
> Call 24Hr Helpline 0300 555 2222 - to safely report a loan shark and to access support/advice about our service.
> Download free STOP LOAN SHARK APP (Google Play/App Store), to report loan sharks and access services. You can also get notified when arrests are made locally, However, you will need your location turned on to access this feature.
Radicalisation
Radicalisation is comparable to other forms of exploitation, such as grooming and child sexual exploitation. Radicalisation’s aim is to attract people to another way of reasoning, inspire new recruits and embed extreme views and persuade vulnerable people of another cause’s legitimacy. This may be through face-to-face encounters or through social media. Most people who commit terrorism offences do so of their own agency and dedication to an ideological cause. There is no single profile of a radicalised person, nor is there a single pathway or ‘conveyor belt’ to being radicalised.
Click on the link below for further information:
Prevent referral form - Liverpool
Liverpool Prevent information guidance
https://www.gov.uk/government/publications/channel-guidance - Prevent pathway Prevent pathway
https://www.counterterrorism.police.uk/
Get help if you’re worried about someone being radicalised - GOV.UK (www.gov.uk)
https://www.gov.uk/report-terrorism
www.gov.uk/prevent-duty-training
https://www.protectuk.police.uk/news-views/protectuk-app
https://www.gov.uk/government/publications/independent-review-of-prevents-report-and-government-response
Liverpool Prevent Referral
PREVENT aims to safeguard individuals at risk of becoming or being drawn into supporting terrorism, by providing early intervention, help and support.
PREVENT referrals can be made by anyone. Any referral of a vulnerable individual who lives within the Liverpool City Council area, should be directed to both Prevent Police and Adult Access simultaneously.
All referrals must be sent, via email, to prevent@merseyside.police.uk.
Prevent referral form - Liverpool - Word document
Liverpool Prevent information guidance - Word document
If you have any other Safeguarding Concerns with regards to this individual please use:
https://liverpool.gov.uk/adult-social-care/worried-about-someone/report-an-adult-at-risk/
Gambling Related Harms
‘Gambling-related harms are the adverse impacts from gambling on the health and wellbeing of individuals, families, communities, and society. These harms impact on people’s resources, relationships, and health.’
Gambling
‘To stake or risk money, or anything of value, on the outcome of something involving chance.’
Gambling related harms can affect anyone. There are some known correlations between some risk factors/presenting behaviours and gambling. These include (but are not limited to):
> Alcohol and Drug Misuse
> Mental ill health
> Domestic Abuse
> High risk of suicide
> Debt/financial difficulties
> Accommodation/Housing difficulties
> Criminal behaviour
> Social isolation
Resources and referral routes
Mini-screening tool for non-specialist services
Self-Assessment tool: Understanding your Relationship with Gambling
Referral form to specialist services with Beacon Counselling Trust – No matter what level of concern you have, Beacon Counselling Trust can triage, support, and offer onward referral with appropriate partners.
2. Talk to the adult (unless it is not safe to do so)
Safeguarding Principle - Protection
What does this mean for the professionals:
Adults are offered ways to protect themselves, and there is a co-ordinated response to adult safeguarding.
What does this mean for the adult:
 I am provided with help and support to report abuse. I am supported to take part in the safeguarding process to the extent to which I want and which I am able. I am provided with help and support to report abuse. I am supported to take part in the safeguarding process to the extent to which I want and which I am able.
|
2.1 Your starting point should be to talk to the adult unless it is not safe to do so
If the adult does not wish to report the abuse consider if they are in immediate danger or at risk of serious harm.
Is the adult experiencing a mental health crisis? If so then see this webpage for further advice on how to respond and Get Help with Mental Health - Help in a crisis (merseycare.nhs.uk)
2.2 Consider if a crime has been committed?
If so, and the adult is in immediate danger or risk of serious harm, then this should be reported to the Police immediately. The adult does not need to give their consent under these circumstances as this would be considered to be in their ‘vital interest’ due to immediate danger or risk of serious harm.
Are others, including children in immediate danger or risk of serious harm? If so, then this should be reported to Police immediately, and consideration also give to reporting this to Children’s Services. The adult(s) does not need to give their consent under these circumstances due to ‘public interest’ considerations.
If there is an immediate safeguarding concern where a child is deemed at risk or has potentially suffered significant harm, children social care should be contacted via the Multi-Agency Referral Form (MARF) or by contacting 0151 233 3700 to discuss the concern if necessary prior to completing the online form. Report a concern about a child in liverpool.gov.uk
Safeguarding and promoting the welfare of children and adults most at risk of abuse and neglect is a shared responsibility. The ‘Think Family’ approach should be used by all practitioners who should consider the needs of the whole family, including young carers, considering family circumstances and responsibilities. Existing professional relationships should be viewed as a chance to identify risk, refer to colleagues in other services, and to use targeted support to help prevent problems from escalating and therefore potentially limiting harm.
Safeguarding Principle - Empowerment
What does this mean for the professionals:
Adults are encouraged to make their own decisions and are provided with information and support.
What does this mean for the adult:
I am consulted about the outcomes I want from the safeguarding process and these directly inform what happens.
|
2.3 Consider if this matter meets the Section 42 (1) criteria within the Care Act 2014 as a Safeguarding Concern:
- do I have reasonable cause to suspect that the adult has needs for care and support; and
- do I have reasonable cause to suspect that the adult is at risk, or experiencing abuse or neglect.
It must be noted that the third criteria (c) under the legal duty for a Section 42 Enquiry (1) is not relevant at the Concern stage:
- because of those needs is unable to protect himself or herself against the abuse or neglect or the risk of it.
SCIE: Assessment and Eligibility Outcomes (Care & Support Needs)
LGA/ADASS Guidance on What Constitutes a Safeguarding Concern - Sept 2020
Local Government Association - What Constitutes a Safeguarding Concern: FAQ's
If there no crime and the criteria to refer a concern appear to have been met, then speak to the adult to get their views on the concern. It is best to support the adult in reporting abuse themselves. Find out what they want to happen next.
If a decision is made not to refer to the Local Authority the individual agency must make a record of the concern and any action taken. Concerns should be recorded in such a way that repeated, low level harm incidents are easily identified and subsequently referred.
Not referring under safeguarding adults’ procedures does not negate the need to report internally or to regulators/commissioners as required. If care providers are using this guidance, it is important to note that all Safeguarding Concerns must be notified to the Local Authority.
If this criteria does not appear to have been met, but you are unsure, then you must seek further advice either from your organisations safeguarding lead or from the Local Authority.
If you are certain that this criteria has not been met, then consider what other pathways, options or services could be used to help support this adult, including providing relevant information. Record your decision-making in an appropriate manner.
2.4 Seek the adult’s consent to submit a Safeguarding Concern to the Local Authority
You should seek the adult’s consent to submit the Safeguarding Concern and explain this may mean that several agencies may gain access to their personal details.
> Read The Eight Caldicott Principles (updated from seven in December 2020).
> Does the adult have the mental capacity to consent to the Safeguarding Concern being submitted now?
> Is there a requirement to provide statutory advocacy.
7 minute briefing Advocacy Liverpool - Word document
2.5 The Care Act 2014 & Advocacy
The Care Act 2014 Statutory Guidance (7.4) states there is a duty to arrange an Independent Advocate for adults to enable those who may otherwise have (1) “substantial difficulty” in being involved if there is (2) “no appropriate individual available to support and represent the person’s wishes”.
The local authority has a duty to instruct an Independent Care Act Advocate if the person meets the criteria above and is going through any of these processes:
> s.9 Needs Assessment.
> s.10 Carer’s Assessment.
> s.25 The preparation of a Care and Support Plan or Support Plan.
> s.27 A review of Care and Support Plan or Support Plan.
> s.42 Safeguarding Enquiry.
> s.44 Safeguarding Adults Review (SAR)
2.6 The Mental Capacity Act 2005 & Advocacy
The Mental Capacity Act Code of Practice Chapter 10 states that:
An IMCA must be instructed, and then consulted, for people lacking capacity who have no-one else to support them (other than paid staff), whenever:
> an NHS body is proposing to provide serious medical treatment, or
> an NHS body or local authority is proposing to arrange accommodation (or a change of accommodation) in hospital or a care home, and the person will stay in hospital longer than 28 days, or – they will stay in the care home for more than eight weeks.
An IMCA may be instructed to support someone who lacks capacity to make decisions concerning:
> care reviews, where no-one else is available to be consulted
> adult protection cases, whether or not family, friends or others are involved
* It is worth noting that there is no provision under The Care Act for advocacy if the person is the alleged perpetrator of abuse or neglect. In this situation, if the person lacks capacity, an IMCA should be instructed.
3. Capacity and consent factors to consider
1. Does the adult have the mental capacity to consent to the Safeguarding Concern being submitted now?
2. Is there any possibility that the adult has/ is suffering from any type of coercion, control, threat, duress or pressure from another person(s) which may mean they refuse consent?
3. Does mental capacity need to be assessed or reviewed?
4. At the concern stage, the most common capacity issues to consider will usually be whether the adult has the mental capacity to make decisions about the abuse or neglect, the related risks, and any immediate safety actions necessary. Another common capacity issue will be whether the adult consents to immediate safety actions being taken, and whether the adult consents to information being referred / shared with other agencies.
5. It is important to establish whether the adult has the mental capacity to make decisions. This may require the assistance of other professionals. In the event of the adult not having capacity, relevant decisions and/or actions must be taken in the person’s best interests. The appropriate decision-maker will depend on the decision to be made.
6. Give due regard to the adult’s views and wishes, including their desired outcomes, including when undertaking Best Interest Decisions in accordance with the Mental Capacity Act.
7. If the adult does have the mental capacity to consent to the Safeguarding Concern being submitted, but refuses, professionals must be careful that they consider how to keep the adult safe if they continue to submit the concern. This may be particularly relevant in domestic abuse cases. The adult must be informed that a Safeguarding Concern has been submitted, unless it is unsafe or impractical to do so.
8. A Safeguarding Concern can still be submitted without the adult’s consent if ‘vital’ or ‘public’ interest considerations apply as outlined above.
9. This means that if a person doesn’t provide consent for a safeguarding concern to be submitted, or requests that information about them is not shared with other safeguarding partners, their wishes should be respected. However, there are a number of circumstances where the practitioner can reasonably override such a decision, including where:
> the person lacks the mental capacity to make that decision – and the referral is considered to be in their best interests this must be properly explored and recorded in line with the Mental Capacity Act as outlined above.
> other people are, or may be, at risk, including children
> sharing the information could prevent a crime
> the person thought to be the cause of risk has care and support needs and may also be at risk
> a serious crime has been committed
> staff are implicated
> the adult has the mental capacity to make that decision, but they may be under duress or being coerced
> the risk is unreasonably high and needs a multi-agency discussion
> a court order or other legal authority has requested the information
If the person does not give their consent then, unless it would increase the risk to them, it should be explained that information will be shared without consent. The reasons should be given and recorded.
The safeguarding principle of proportionality should underpin decisions around sharing information without consent, and decisions should be on a case-by-case basis.
If it is not clear that information should be shared outside the organisation, a conversation can be had with safeguarding partners in the police or local authority without disclosing the identity of the person in the first instance. They can then advise on whether full disclosure is necessary without the consent of the person concerned.
For more information read:
LGA/ADASS Guidance on What Constitutes a Safeguarding Concern - Sept 2020
4. Gather as much information as possible
Having spoken to the adult (as above) and determined their views, wishes and desired outcomes. Also gather as much information as possible from other relevant sources and documentation:
Does anyone else need to be informed or involved, including the nominated safeguarding lead in your agency, before progressing to submitting a Safeguarding Concern?
> Are there any other internal policy or procedural requirements within your agency?
> If you unhappy about how your organisation is dealing with a Safeguarding Concern do you know how to escalate this, which could include the use of a Whistleblowing Policy?
See our guidance on identifying and responding to safeguarding concerns here: https://liverpoolsab.org/professionals/local-policies-and-procedures/
5. Submit the Adult Safeguarding Concern
> Ensure all of the relevant fields in the Safeguarding Concern form (please use the ‘report an adult at risk form’ on liverpool.gov.uk on liverpool.gov.uk) are fully completed with as much detail as possible, and submitted correctly using the contact details outlined in the link below.
> You should receive receipt of this and be kept informed of progress.
> If you do not receive any feedback on progress you should follow this up with the Local Authority involving your organisational lead if required, and in exceptional circumstances this can also be escalated to the Liverpool Safeguarding Adults Board to consider.
Be aware of Liverpool SAB’s Resolving Professional Differenced and Escalation Process: https://liverpoolsab.org/professionals/local-policies-and-procedures/
6. Allegations against People in Positions of Trust (PiPOT)
Liverpool City Council’s ‘relevant partners’ (outlined in the Care Act), and those providing universal care and support services, should have clear policies for dealing with allegations against people who work, in either a paid or unpaid capacity, with adults with care and support needs.
Where such concerns are raised about someone who works with adults with care and support needs, it will be necessary for the employer (or student body or voluntary organisation) to assess any potential risk to adults with care and support needs who use their services, and, if necessary, to take action to safeguard those adults.
If the allegation and the circumstances of it matches the criteria outlined above, then the guidance for submitting a Safeguarding Concern to the Local Authority should be followed. The guidance for the Local Authority in conducting Safeguarding Enquiries (on the following pathway pages) outline the possible outcomes that may be relevant in such cases.
Whilst the focus of safeguarding adults work is to safeguard one or more identified adults with care and support needs (adult at risk), there are occasions when incidents are reported that do not involve an adult at risk, but indicate, nevertheless, that a risk may be posed to adults at risk by a person in a position of trust.
Examples of such concerns could include allegations that relate to a person who works with adults with care and support needs who has:
> Behaved in a way that has harmed or may have harmed an adult or child (this could include their own family members).
> Possibly committed a criminal offence against, or related to, an adult or child.
> Behaved towards an adult or child in a way that indicates they may pose a risk of harm to adults with care and support needs.
When a person’s conduct towards an adult may impact on their suitability to work with or continue to work with children, this must be referred to the Local Authority’s Designated Officer (LADO).
Employers, student bodies and voluntary organisations should have clear procedures in place setting out the process, including timescales, for investigation and what support and advice will be available to individuals against whom allegations have been made. Any allegation against people who work with adults should be reported immediately to a senior manager within the organisation. Employers, student bodies and voluntary organisations should have their own sources of advice (including legal advice) in place for dealing with such concerns.
If an organisation removes an individual (paid worker or unpaid volunteer) from work with an adult with care and support needs (or would have, had the person not left first) because the person poses a risk of harm to adults, the organisation must make a referral to the Disclosure and Barring Service. It is an offence to fail to make a referral without good reason.
6.1 Disclosure and Barring Service (DBS) Briefing
If there any concerns about the behaviour and conduct of a professional working with an adult at risk of abuse and neglect, then this should be reported as a Safeguarding Concern under the ‘Public Interest Duty’, and if this work is a regulated activity, then a referral to the Disclosure and Barring Service (DBS) should also be considered:
DBS Briefing
In some instances, a relevant agency may come across information about a person in a position of trust who does not work or volunteer for them, and feel it is appropriate to notify the local authority outside of the formal adult safeguarding procedures.
Decisions on sharing information must be justifiable and proportionate, based on the potential or actual harm to adults or children at risk and the rationale for decision-making should always be recorded.
Care Act 2014 - Care and Support Statutory Guidance: 14.120 to 14.132
Principals to Inform PiPOT - National Safeguarding Adults Network
ADASS - Top Tips for Dealing with Allegations for PiPOT
See Liverpool PIPOT protocol and North West PIPOT Procedure: https://liverpoolsab.org/professionals/local-policies-and-procedures/
7. Safeguarding Standards
These adult safeguarding procedures share safeguarding standards. Adhering to timescales should reflect the ethos of the Making Safeguarding Personal agenda. It is important that timely action is taken, whilst respecting the principle that the views of the adult at risk are paramount. It is the responsibility of all agencies proactively to monitor concerns to ensure that drift does not prevent timely action and place people at further risk.
Divergence from any target timescales may be justified where:
> Adherence to the agreed timescales would jeopardise achieving the outcome that the adult at risk wants;
> It would not be in the best interests of the adult at risk;
> Significant changes in risk are identified that need to be addressed;
> Supported decision making may require an appropriate resource not immediately available;
> Persons’ physical, mental and/or emotional wellbeing may be temporarily compromised. The timescales need to reflect:
> All other investigations such as PSIRF need to take place before conclusion.
Safeguarding concerns - Incoming concerns will be screened within 4 working hours or within the same day of receipt.
The aim will be for all Safeguarding concerns to be triaged within 2 working days
If the person themselves is not seen or spoken to during the concern stage – there is to be a record within the concern of why.
Immediate safety plan to be confirmed at concern stage.
Safeguarding Enquiries - Enquiry planning to be completed within 2 days of receipt or sooner should the level of risk indicate a more urgent response – review of immediate safety planning to take place during these discussions.
Enquiry planning meetings (when required) to be completed within 5 days of receipt or sooner depending on the level of risk – Same day enquiry planning meetings can be held. Enquiry planning meetings should not be limited to the start of the enquiry, and can be held at any point during the enquiry where the need for a meeting arises.
Enquiry – within 28 days where possible but no longer than 3 months.
Safeguarding plan – within 28 days (same time as enquiry to be completed).
Safeguarding plan review – to be completed as and when required dependent on risk no more than 3 months. Within 3 months the actions within safeguarding plan review would generally be incorporated into the care and support plan if these actions are still required.
Safeguarding Assessments and Reviews - Needs Assessment / Review (s11 Care Act 2014) to be completed alongside the enquiry where required, with the same 28-day target
Enquiry closure - Immediately following the decision to close, but all actions completed and closure on Liquid Logic within 5 working days of the decision to close.
8. Guidance for Making Decisions on the duty to carry out adult safeguarding enquiries
This section has been developed to assist practitioners in assessing the context, seriousness and level of risk associated with an adult safeguarding concern, and in doing so, help with the consistency of decision making used to cause a safeguarding enquiry to be conducted. It is primarily for use by lead professionals working in the Local Authority at the point of receiving an adult safeguarding concern; although others may also find it helpful to refer to this guidance when responding to a concern of abuse or neglect, and deciding if this should be referred to, the Local Authority. If care providers are using this guidance, it is important to note that all Safeguarding Concerns must be notified to the Local Authority.
8.1 Legal definitions
The Care Act 2014 statutory guidance and Section 42 (1) criteria states that the Local Authority must make enquiries, or cause others to do so, if they reasonably have cause to suspect an adult:
- Has needs for care and support (whether or not the local authority is meeting any of those needs) and;
- Is experiencing, or at risk of, abuse and neglect; and
- As a result of those care and support needs is unable to protect themselves from either the risk of, or the experience of abuse or neglect.
Referring agencies need to use their professional judgement, consider the views of the adult at risk, and where appropriate seek consent for sharing information on a multi-agency basis.
8.2 Managing the different levels of harm
In order to manage the large volume of adult Safeguarding Concerns which come under safeguarding adults’ policy and procedures, there is a need to differentiate between those concerns relating to low level harm/risk, and those that are more serious. Whilst it is likely that concerns relating to low level harm/risk will not progress beyond an Initial Enquiry Stage, the concern will be recorded by the Local Authority and proportionate action taken to manage the risks that have been identified. This may include: provision of information or advice; referral to another agency or professional; assessment of care and support needs.
The sharing of low level concerns helps the Local Authority to understand any emerging patterns or trends that may need to be taken into consideration when deciding whether safeguarding adults procedures need to continue.
Other guidance you may find helpful is included below:
Local Government Association - Making Safeguarding Personal Toolkit
LGA/ADASS Guidance on What Constitutes a Safeguarding Concern - Sept 2020
LGA/ADASS Making Decisions on the Duty to Carry out a Safeguarding Enquiry
The guidance is not designed in a way in which further actions are determined by achieving a score, it is there to provide guidance and key considerations for practitioners who are assessing the context, circumstances, seriousness and impact of the abuse that is occurring, as well as the risk of it recurring.
8.3 Non-Statutory Safeguarding Enquiry
What does this mean for the professionals: A proportionate and least intrusive response is made balanced with the level of risk.
What does this mean for the adult:
I am confident the professionals will work in my interest and only get involved as much as needed.
Other Safeguarding Enquiries can be used when all of the Section 42 (1) criteria have not been met (see section 2), but the Local Authority still considers it “necessary and proportionate” to conduct a safeguarding enquiry. This could be linked to promoting an individual’s well-being as outlined in Section 1 of the Care Act, or for carers who do not qualify under Section 42.
Examples of where the local authority may still choose to undertake a non-statutory safeguarding enquiry could be when a carer is considered to be at risk of abuse and / or neglect, allegations of forced marriage, female genital mutilation and honour based abuse.
Safeguarding Principle - Proportionality
Concerns around modern slavery, or high risk ongoing domestic abuse where the person at risk appears to have support needs should also be considered.
|
8.4 Dealing with historic allegations of abuse where the adult is no longer at risk
One of the criteria for undertaking statutory enquiries under the Care Act Section 42 duty is that the adult is experiencing or is at risk of, abuse or neglect. Therefore, the duty to make enquiries under the Care Act relates to abuse or neglect, or a risk of abuse or neglect that is current or where there is a potential risk of them experiencing abuse or neglect in the future.
Concerns relating to historic abuse or neglect, where the person is no longer at risk will be considered to determine whether they demonstrate a current or potential risk of harm to other adults and also whether they require criminal or other enquiry through parallel processes (for example complaints, inquests, regulatory, commissioning, non-statutory enquiry, health and safety investigations etc).
8.5 The interface between Section 42 Enquiries and Safeguarding Adults Reviews (SAR)
As a matter of law an enquiry under Section 42 cannot be initiated in relation to an adult who is deceased. However, if the circumstances of the death mean that there are reasons to be concerned about risks to other adults, Section 42 Enquiries may need to be made to decide whether action needs to be taken to protect those other adults. For example, this will often be necessary following a death in an organisational setting where other adults are continuing to receive a service.
Where a Section 42 Enquiry has already commenced and the adult subsequently passes away then, the enquiry may need to continue if there are potential ongoing transferrable risks to other adults. Otherwise, a multi-agency decision, which could include family members, should be made regarding the enquiry potentially being concluded if no transferrable risks are identified.
Where a death is suspected to be the result of abuse or neglect and the other SAR criteria are met, a SAR notification should be submitted to enable the Liverpool Safeguarding Adults Board (LSAB) to consider this under Section 44 of the Care Act. Please follow your own agencies internal processes around making SAR referrals to the Board, this would usually be via your agencies safeguarding lead.
How to make a SAR Referral to the Liverpool Safeguarding Adults Board
https://liverpoolsab.org/professionals/safeguarding-adults-reviews/
You can also find Liverpool Safeguarding Adults Board SAR Protocol here
Please find Liverpool SAR Protocol:
https://liverpoolsab.org/professionals/local-policies-and-procedures/
The Care Act statutory guidance gives examples of serious abuse or neglect cases where an adult “would have been likely to have died but for an intervention or has suffered permanent harm or has reduced capacity or quality of life (whether because of physical or psychological effects) as a result of the abuse or neglect”. Under these circumstances, Section 42 Enquiries into what happened to that adult will still need to take place, to ensure the adult’s immediate safety and the safety of any others who may be at risk but should be limited to those purposes rather than duplicating a more thorough review into the history which may take place through a SAR.
The Local Authority (or delegated agency) may need to make initial enquiries to consider whether the conditions for a SAR are met, but should not describe these as Section 42 Enquiries. In these circumstances any discussions or meetings that take place can be logged onto the case management system along with the decision making as to whether a SAR referral is made.
Where the suspected abuse or neglect has taken place in an organisational setting, and there may be potential risks to others, consideration for an organisational safeguarding process should be considered. Guidance for Organisational Safeguarding will be available later in 2025.
9. Factors to be considered when deciding whether the duty to undertake a safeguarding enquiry is triggered.
9.1 Contextual Factors
The following table should be used to consider the context of the Safeguarding Concern alongside the broader issues such as: mental capacity; mental health; physical disability; learning disability; communication issues; possible coercive control and the relationship between the adult and any person alleged to have caused harm; where the adult lives; who do they rely upon for their care; what is the extent of their circle or network of supportive relationships.
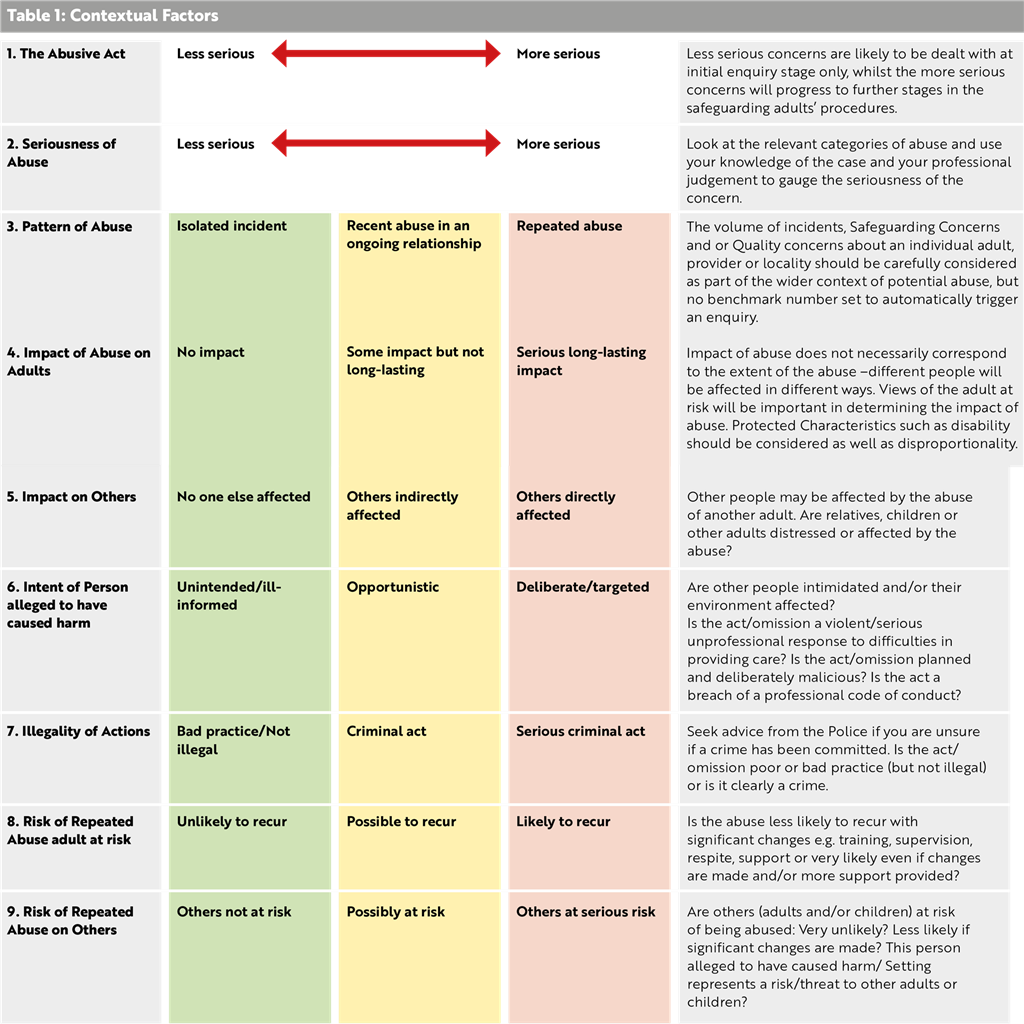
9.2 Types and Level of Abuse
Our guidance on identifying and responding to safeguarding concerns should be used in conjunction with table 1 above. The issues described in the amber section may be notified to the Local Authority, but these could be managed at the Concern stage and may not progress to a safeguarding enquiry, depending on what other information is available.
Concerns of a more serious nature should be referred to the Local Authority.
These concerns will receive additional scrutiny and progress further under Safeguarding Adults’ procedures. Where a criminal offence is thought or alleged to have been committed the Police will be contacted. Other emergency services should be contacted as required.
9.3 Sharing the outcome of safeguarding concerns.
All adult safeguarding concerns referred to the Local Authority should be assessed to decide if the criteria for adult safeguarding are met. Keeping a professional who raised the concern informed is an essential requirement under these procedures. Feedback provides assurance that action has been taken whether under adult safeguarding or not. Organisations raising concerns may want to challenge or discuss decisions and need to be updated on what action has been taken. Feedback to members of the public and the wider community needs to take account of confidentiality and requirements of data protection legislation.
9.4 Dealing with repeat allegations / concerns
All concerns should be considered on their own merit and recorded individually. An adult who makes repeated allegations that have been investigated and decided to be unfounded should be treated without prejudice. Where there are patterns of similar concerns being raised by the same adult within a short time period, a risk assessment and risk management plan should be developed, and a local process agreed for responding to further concerns of the same nature from the same adult. All organisations are responsible for recording and noting where there are such situations and may be asked to contribute to a multi-agency response. Information sharing to assess and analyse data is essential to ensure that adults are safeguarded, and an appropriate response is made. Staff should also be mindful of public interest issues.
In considering how to respond to repeated concerns the following factors need to be considered:
> The safety of the adult who the concern is about;
> Mental capacity and ability of the individual’s support networks to raise the concern, or to increase support to meet outcomes of safeguarding concerns;
> Wishes of the adult at risk and impact of the concern on them;
> Impact on important relationships;
> Level of risk.
9.5 Professional differences and escalation
Professional differences should be resolved at the earliest opportunity, ensuring that the safety and wellbeing of the adult at risk remains paramount. Challenges to decisions should be respectful and resolved through co-operation. Disagreements can arise in a number of areas and staff should always be prepared to review decisions and plans with an open mind. Assurance that the adult at risk is safe takes priority. Disagreements should be talked through and appropriate channels of communication established to avoid misinterpretation. In the event that operational staff are unable to resolve matters, more senior managers should be consulted. Multi-agency network meetings may be a helpful way to explore issues with a view to improving practice. In exceptional circumstances or where it is likely that partnership protocols are needed the SAB should kept appraised of the issues and agree what type of evaluation will be undertaken. In the case of care providers, unresolved disputes should be raised with the relevant managers leading on the concern and commissioners.
See our Resolving Professional Differences and Escalation procedure for more information: https://liverpoolsab.org/professionals/local-policies-and-procedures
9.6 Cross-boundary and inter-authority adult safeguarding enquiries
Risks may be increased by complicated cross-boundary arrangements, and it may be dangerous and unproductive for organisations to delay action due to disagreements over responsibilities. The rule for managing safeguarding enquiries is that the Local Authority for the area where the abuse occurred has the responsibility to carry out the duties under Section 42 Care Act 2014, but there should be close liaison with the placing authority. The ‘placing Local Authority’ continues to hold responsibility for commissioning and funding a placement. However, many people at risk live in residential settings outside the area of the placing authority. In addition, a safeguarding incident might occur during a short-term health or social care stay, or on a trip, requiring police action in that area or immediate steps to protect the person while they are in that area.
The initial lead in response to a safeguarding concern should always be taken by the Local Authority for the area where the incident occurred. This might include taking immediate action to ensure the safety of the person or arranging an early discussion with the police when a criminal offence is suspected. Further action should then be taken in line with Making Safeguarding Personal on the views of the adult, and the Care and Support statutory guidance on who is best placed to lead on an enquiry.